Empowering Teens to Build Healthy Relationships
February 2, 2026
February is Teen Dating Violence Prevention Month, a time to shine a light on an issue affecting far too many young people.
February is Teen Dating Violence Prevention Month, a time to shine a light on an issue affecting far too many young people.
With Gratitude and Anticipation for the Great Work Ahead, Dr. Jennifer Thomas
With Gratitude and Anticipation for the Great Work Ahead, Dr. Jennifer Thomas
With Gratitude and Anticipation for the Great Work Ahead, Dr. Jennifer Thomas
With Gratitude and Anticipation for the Great Work Ahead, Dr. Jennifer Thomas
With Gratitude and Anticipation for the Great Work Ahead, Dr. Jennifer Thomas
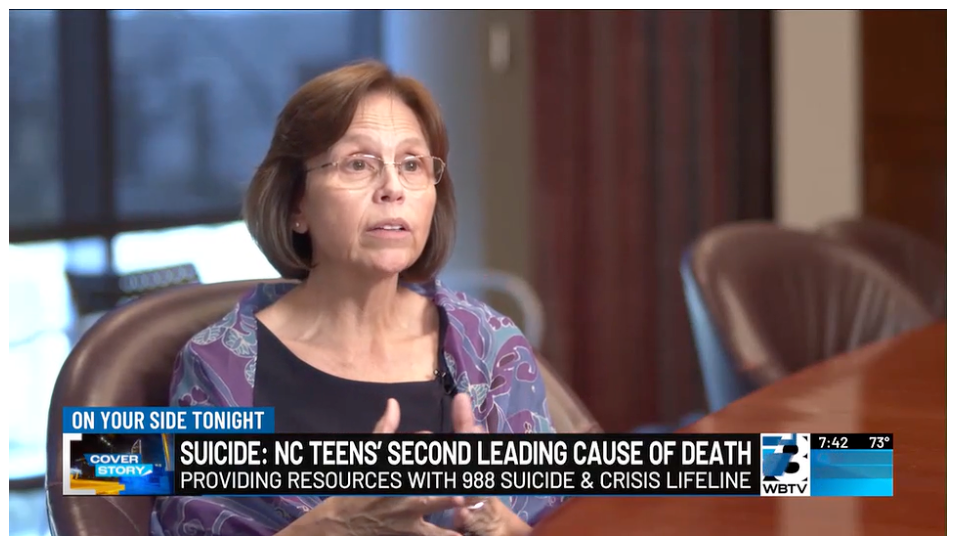
CHARLOTTE, N.C.- 988 Day is an annual day of action to raise awareness about the 988 suicide and crisis lifeline. Libby Safrit, Executive Director and Clinical psychologist at Teen Health Connection chats about the importance of the day.


At Teen Health Connection, we believe that helping teens thrive really begins at home with their parents and caregivers. Our Health Education team works alongside parents of teens and adolescents to strengthen relationships, build communication, and set consistent boundaries—all key elements when supporting adolescents through change and challenge. They do this through workshops and training sessions and establishing a presence in the community while sharing information. Get to know Kris N. Hawkins, our parent education coordinator and Kenyatta “Dr. Ken” O’Bryant, Ph.D., manager of health education and community outreach.
Meet Kris N. Hawkins, our Parent Education Coordinator, who has been with Teen Health Connection for six years. Kris coaches parents of teens and young children using evidence-based practices. Her work focuses on 45-minute to 1-hour trainings that teach parents how to establish healthy relationships and provide strategies on how to communicate with their children calmly and respectfully. “I came to Teen Health Connection when my oldest was 17 and found the resources I needed. I consider it a privilege to be able to do that for others today,” she shares.
Using the active parenting of teens approach, Kris demonstrates the benefits of adopting authoritative parenting principles, which encourage parents to show up for their teen in a loving, respectful way and provide consistent boundaries. It is an evidence-based approach that shows that teens parented this way are less likely to struggle with anxiety, depression, or academic problems.
Kris hosts workshops throughout the city and county, often partnering with local organizations to reach a broader audience. She also provides support to families in transitional housing through strategic relationships with Families Forward and Charlotte Family Housing. While she may not work directly with families experiencing housing insecurity or homelessness, she knows that her efforts provide some support in a highly stressful situation and offers access to helpful resources. “My role is to empower parents, focus on their strengths, and help them feel seen by designing sessions that are flexible and accessible. Once you’ve found us, you have a resource for life,” Kris says.
“My goal is for parents to feel more confident after they attend a training and to recognize they are not alone. “I always try to stress to parents that I will always be a resource for them. They have all my contact information. They don’t feel like I am on a pedestal. I share my parenting struggles with them and they feel as though I’m in the trenches just like them,” she shared. “Yes, I’m an expert on the parenting material, but there is no “parenting expert or perfect parent,” she concludes.

Kris N. Hawkins, Parent Education Coordinator
Another element of the health education team is community outreach, and that’s where Dr. Kenyatta O’Bryant comes in. “Dr. Ken,” recently joined the team, having previously served as the Deputy Director of Homeless Services for the city of Baltimore, Maryland. In that role he oversaw programs for youth ages 14 to 25 who faced housing insecurity and behavioral health challenges.
Now, at Teen Health Connection, Dr. Ken and his team collaborate with local hospitals, schools, and nonprofit partners to empower and inform parents about the organization’s behavioral health services. “We are the backbone of Teen Health Connection when it comes to adolescent and behavioral health,” Dr. O’Bryant explains. “As health educators, our job is to engage the community—internally and externally—and provide people with the information and resources they need to make informed decisions based on what’s available to them.”
Dr. Ken ensures that he educates parents through a health equity lens to ensure that information is accessible to all. “Our goal is to give people information and resources to make informed decisions,” he shares.
The mission of the community outreach team is to be a holistic resource for families of teens. “We educate the community not only about adolescent and behavioral health but also about the totality of wellness—chronic disease, mental health, prevention, and overall well-being. Our role is to help people live healthier lives and understand what good health really means,” Dr. Ken concludes.

Kenyatta S. O’Bryant, Ph.D., Manager of Health Education and Community Outreach
Another key member of the Health Education team is Madi Davis, health educator and teens program coordinator. Next month’s newsletter will feature more about Madi’s work with our teens through the Teen Advisory Board, Teen Leadership Summits, our Johnston Ziegler Safrit Youth Leadership scholarship and more.

Madi Davis, health educator and teens program coordinator

Often, when we think of homelessness, we picture someone living on the streets or in a shelter with other unhoused individuals. However, for teens and adolescents, housing insecurity can look different.
This month, our health education topic is Teen Homelessness Awareness and Prevention, and we want to help you recognize the signs if you encounter a young person who may be experiencing housing insecurity. According to our community partner Families Forward, approximately 45,000 children are experiencing poverty right here in Charlotte. In the Charlotte-Mecklenburg Housing and Homelessness dashboard, the article on The Rising Challenge of Student Homelessness states that during the 2024-2025 school year, Charlotte-Mecklenburg Schools (CMS) identified a total of 5,680 students experiencing homeless, an 18% increase from the 4,815 students identified during the 2023–2024 school year.
This increase isn’t just a statistic; it reflects the rising housing instability impacting families with minor children across our community. Research shows that poverty is a major contributor to youth homelessness, which means there is a high probability that someone in your sphere of influence may be at risk of not having consistent shelter. Many young people experiencing homelessness aren’t on the streets — they’re moving from one friend’s or relative’s home to another, unsure where they’ll sleep next. For some, age restrictions prevent them from staying in shelters with their parents or guardians. For others, family conflict or lack of support leaves them without a stable place to call home.
A Closer Look at Who’s Affected
Certain groups face even greater barriers. LGBTQ+ teens often experience rejection and have fewer safe spaces to turn to, while teens with children and youth aging out of foster care are at particularly high risk. At that age, the stigma surrounding homelessness can make it hard for teens to ask for help, but here’s what you need to know. This issue is closer than we think and the degrees of separation between stability and homelessness have never been smaller.
A Local Perspective
Given Charlotte’s record as 38th nationwide for economic mobility and knowing that access to affordable housing is a major lever in this process, homelessness can trap multiple generations in financial insecurity if not addressed. Poverty isn’t new in our community — and that’s part of the challenge. Without collective awareness and action, the problem persists.
To help raise awareness about this growing problem, Mecklenburg County has launched a 100-Day Challenge to Prevent Youth Homelessness. Visit the website to learn more.
Here at Teen Health Connection, we work holistically to prepare teens for life’s challenges and connect them to essential community partners such as Charlotte Family Housing and Families Forward, both of which are saving families from homelessness every day. This November, we encourage parents, caregivers, and community members to recognize the signs, build empathy, and share this message. This newsletter is filled with information and suggestions on how you can help make a difference.
Together, we can raise awareness and help more teens find safety, stability, and hope.
Resources for Teens & Families
Remember, help is just a phone call or email away. Contact a member of our team at: TeenHealthConnection@TeenHealthConnection.org or call (704) 381-8336.
Teen Health Connection has placed billboards and electronic signs like the one above throughout Mecklenburg County highlighting our behavioral health services.